Fillable Nyc Pba 14 Form in PDF
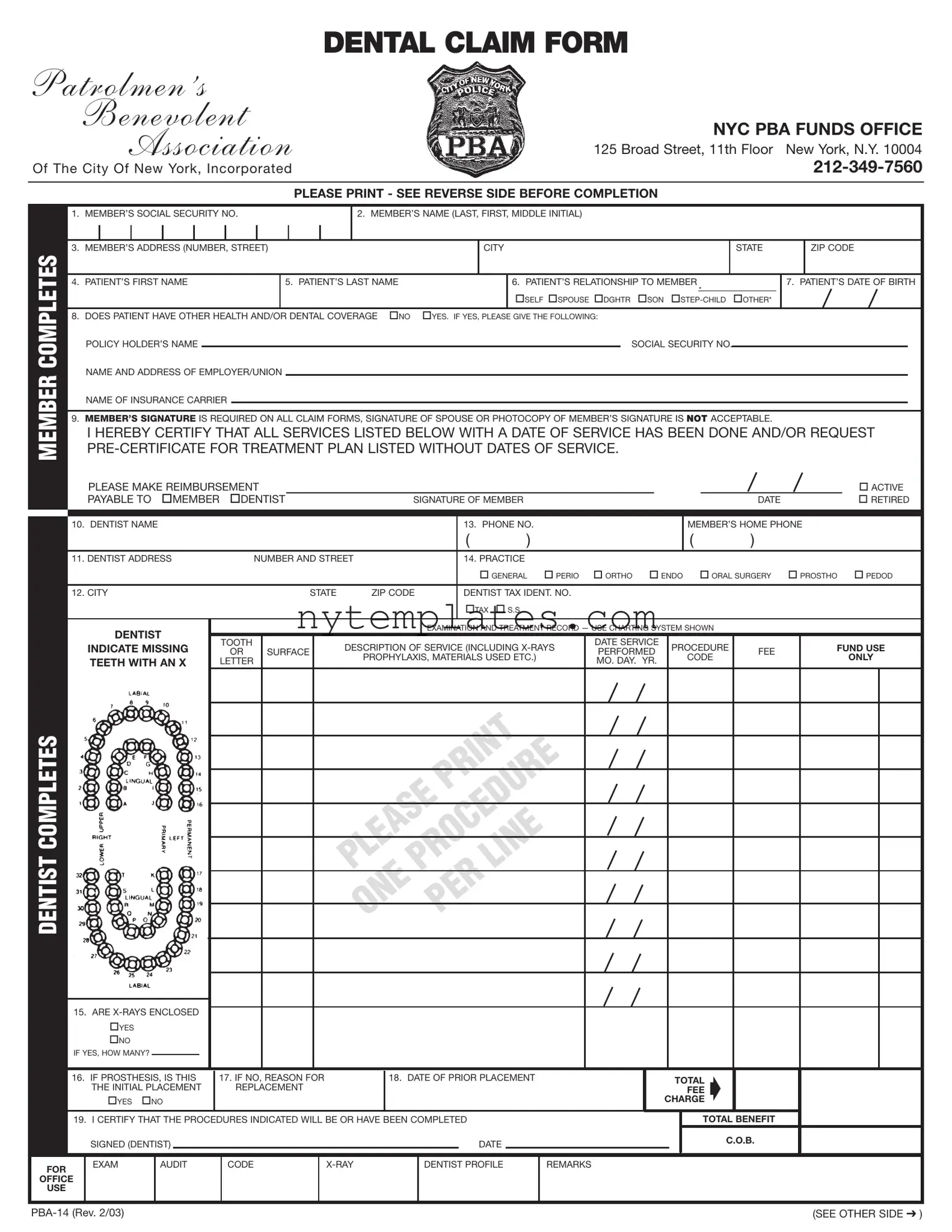
The NYC PBA 14 form serves as a crucial tool for members of the Patrolmen’s Benevolent Association seeking dental benefits. This form facilitates the submission of dental claims, ensuring that members receive appropriate reimbursements for dental services rendered. It requires essential information, such as the member's social security number, name, and contact details, as well as specifics about the patient, including their relationship to the member and date of birth. The form also prompts members to disclose any additional health or dental coverage, which is vital for coordinating benefits. A signature from the member is mandatory, underscoring the importance of accuracy and accountability in the claims process. Additionally, the form outlines requirements for precertification for certain procedures, such as crowns and orthodontics, highlighting the need for members to communicate effectively with their dental providers. By following the instructions provided, members can navigate the claims process smoothly and ensure that they receive the benefits they are entitled to.
Preview - Nyc Pba 14 Form
|
|
DENTAL CLAIM FORM |
PATROLMEN ’S |
|
|
|
BENEVOLENT |
NYC PBA FUNDS OFFICE |
|
ASSOCIATION |
|
|
125 Broad Street, 11th Floor New York, N.Y. 10004 |
|
|
Of The City Of New York, Incorporated |
|
|
|
|
|
|
|
|
|
PLEASE PRINT - SEE REVERSE SIDE BEFORE COMPLETION |
MEMBER COMPLETES
1. |
MEMBER’S SOCIAL SECURITY NO. |
|
|
|
2. MEMBER’S NAME (LAST, FIRST, MIDDLE INITIAL) |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
MEMBER’S ADDRESS (NUMBER, STREET) |
|
|
|
|
|
|
CITY |
|
STATE |
|
ZIP CODE |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
PATIENT’S FIRST NAME |
|
5. PATIENT’S LAST NAME |
|
|
|
6. PATIENT’S RELATIONSHIP TO MEMBER |
|
7. PATIENT’S DATE OF BIRTH |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF SPOUSE DGHTR SON |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
DOES PATIENT HAVE OTHER HEALTH AND/OR DENTAL COVERAGE |
NO |
YES. IF YES, PLEASE GIVE THE FOLLOWING: |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
POLICY HOLDER’S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY NO. |
|
|
|
|
|
||||
|
NAME AND ADDRESS OF EMPLOYER/UNION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9. |
MEMBER’S SIGNATURE IS REQUIRED ON ALL CLAIM FORMS, SIGNATURE OF SPOUSE OR PHOTOCOPY OF MEMBER’S SIGNATURE IS NOT ACCEPTABLE. |
|
|
|
||||||||||||||||||||
I HEREBY CERTIFY THAT ALL SERVICES LISTED BELOW WITH A DATE OF SERVICE HAS BEEN DONE AND/OR REQUEST
|
|
PLEASE MAKE REIMBURSEMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACTIVE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
PAYABLE TO |
MEMBER |
DENTIST |
|
SIGNATURE OF MEMBER |
|
|
|
|
|
|
DATE |
|
RETIRED |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. DENTIST NAME |
|
|
|
|
|
|
|
|
13. PHONE NO. |
|
|
|
|
MEMBER’S HOME PHONE |
|
||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
( |
|
) |
|
|
|
|
11. DENTIST ADDRESS |
|
|
|
NUMBER AND STREET |
|
|
14. PRACTICE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
GENERAL |
PERIO |
ORTHO |
ENDO |
ORAL SURGERY |
PROSTHO |
PEDOD |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
12. CITY |
|
|
|
|
|
STATE |
ZIP CODE |
|
DENTIST TAX IDENT. NO. |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
TAX |
S.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
DENTIST |
|
|
|
|
|
|
|
EXAMINATION AND TREATMENT RECORD — USE CHARTING SYSTEM SHOWN |
|
|
|
||||||||
|
|
|
|
TOOTH |
|
|
DESCRIPTION OF SERVICE (INCLUDING |
|
DATE SERVICE |
PROCEDURE |
|
FUND USE |
|||||||||
|
|
INDICATE MISSING |
|
|
|
|
|||||||||||||||
|
|
OR |
SURFACE |
|
PERFORMED |
FEE |
|||||||||||||||
|
|
|
|
|
|
PROPHYLAXIS, MATERIALS USED ETC.) |
|
|
CODE |
|
ONLY |
||||||||||
|
|
TEETH WITH AN X |
LETTER |
|
|
|
|
MO. DAY. YR. |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
COMPLETES |
|
||
|
|
LINE |
|
|
|
|
|
DENTIST |
PLEASEPROCEDURE |
||
ONE |
PER |
|
|
|
|
|
|
|
15. ARE |
|
|
|
YES |
|
|
|
NO |
|
|
|
IF YES, HOW MANY? |
|
|
|
|
16. IF PROSTHESIS, IS THIS |
17. IF NO, REASON FOR |
|
18. DATE OF PRIOR PLACEMENT |
|
TOTAL |
|||||||||||
|
|
|
THE INITIAL PLACEMENT |
|
REPLACEMENT |
|
|
|
|
|
|
|
FEE |
|||||
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
CHARGE |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
19. I CERTIFY THAT THE PROCEDURES INDICATED WILL BE OR HAVE BEEN COMPLETED |
|
|
TOTAL BENEFIT |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C.O.B. |
|
|
|
|
SIGNED (DENTIST) |
|
|
|
|
|
|
|
DATE |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR |
|
EXAM |
|
AUDIT |
|
CODE |
|
|
DENTIST PROFILE |
REMARKS |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
OFFICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
USE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(SEE OTHER SIDE ) |
INSTRUCTIONS
PRECERTIFICATION IS REQUIRED FOR ALL CROWN AND BRIDGE, PROSTHETIC, ORTHODONTIC, AND PERIODONTIC WORK.
DENTIST:X-RAYS MUST BE SUBMITTED WITH ALL CLAIMS REQUESTING PRECERTIFICATION.
STUDY MODELS ARE ALSO REQUIRED FOR ALL
ORTHODONTIC CLAIMS.
PERIO CHARTING IS REQUIRED FOR ALL
PERIODONTIC CLAIMS
MEMBER:DO NOT ALLOW YOUR DENTIST TO COMMENCE ANY PROCEDURES WHERE PRECERTIFICATION IS REQUIRED UNTIL BOTH YOU AND YOUR DENTIST HAVE RECEIVED THE PRECERTIFICATION.OTHERWISE, YOU WILL BE LIABLE FOR PAYMENT OF SERVICES THAT MIGHT NOT BE APPROVED BY THE PLAN.
NOTE:ALL COMMUNICATIONS WITH THE FUNDS OFFICE MUST INCLUDE PATIENTS CLAIM NUMBER (WHEN KNOWN) OR MEMBERS SOCIAL SECURITY NUMBER.
IMPORTANT: FOR PROTECTION OF YOURSELF AND THE PBA FUNDS, PLEASE DO NOT SIGN BOX #9 ON THE FRONT OF THIS FORM UNTIL THOSE SERVICES ACTUALLY ARE PERFORMED OR THOSE REQUIRING PRECERTIFICATION HAVE BEEN
ALL CLAIMS SUBJECT TO REVIEW FOR COORDINATION OF BENEFITS
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | The NYC PBA 14 form is a Dental Claim Form used by members of the Patrolmen's Benevolent Association to request reimbursement for dental services. |
| Member Information | Members must provide their Social Security number, name, and address on the form to ensure proper identification and processing of claims. |
| Patient Details | The form requires information about the patient, including their name, relationship to the member, and date of birth. |
| Other Coverage | If the patient has other health or dental insurance, details about the policy holder and insurance carrier must be included. |
| Signature Requirement | The member's signature is necessary on the claim form. A spouse's signature or a photocopy of the member's signature is not acceptable. |
| Dental Provider Information | Details about the dentist, including their name, address, and phone number, are required to process the claim effectively. |
| X-Ray Submission | X-rays must be submitted with all claims that request precertification, ensuring that all necessary documentation is provided. |
| Precertification Requirement | Precertification is mandatory for specific dental procedures, such as crowns and orthodontics, to avoid unexpected costs for the member. |
| Communication | All communications with the PBA Funds Office should include the patient's claim number or the member's Social Security number for efficient processing. |
More PDF Templates
Nyc Rent Tax Return - Procedure for accurately reporting New York City Real Property Tax escalations and credits.
Nyc Ubt - Interest, additional charges, and penalties related to underpayment of estimated tax must be calculated if applicable.