Fillable Nyc Buildings Elv1 Form in PDF
The NYC Buildings ELV1 form is a crucial document for anyone involved in the installation, alteration, or removal of elevators and related devices within New York City. This form requires detailed information about the elevator application, including the type of work being performed, whether it involves a new installation, an alteration, or a dismantling of existing equipment. Applicants must provide their contact details, including the name and license of the filing representative, as well as comprehensive information about the building's location and ownership. The form also collects specifics about the elevator device itself, such as its type, capacity, and safety features. Additionally, it includes sections dedicated to insurance information and a declaration of work description. Proper completion of the ELV1 form is essential, as inaccuracies can lead to delays or penalties. By ensuring that all required information is accurately provided, applicants can facilitate a smoother approval process and maintain compliance with city regulations.
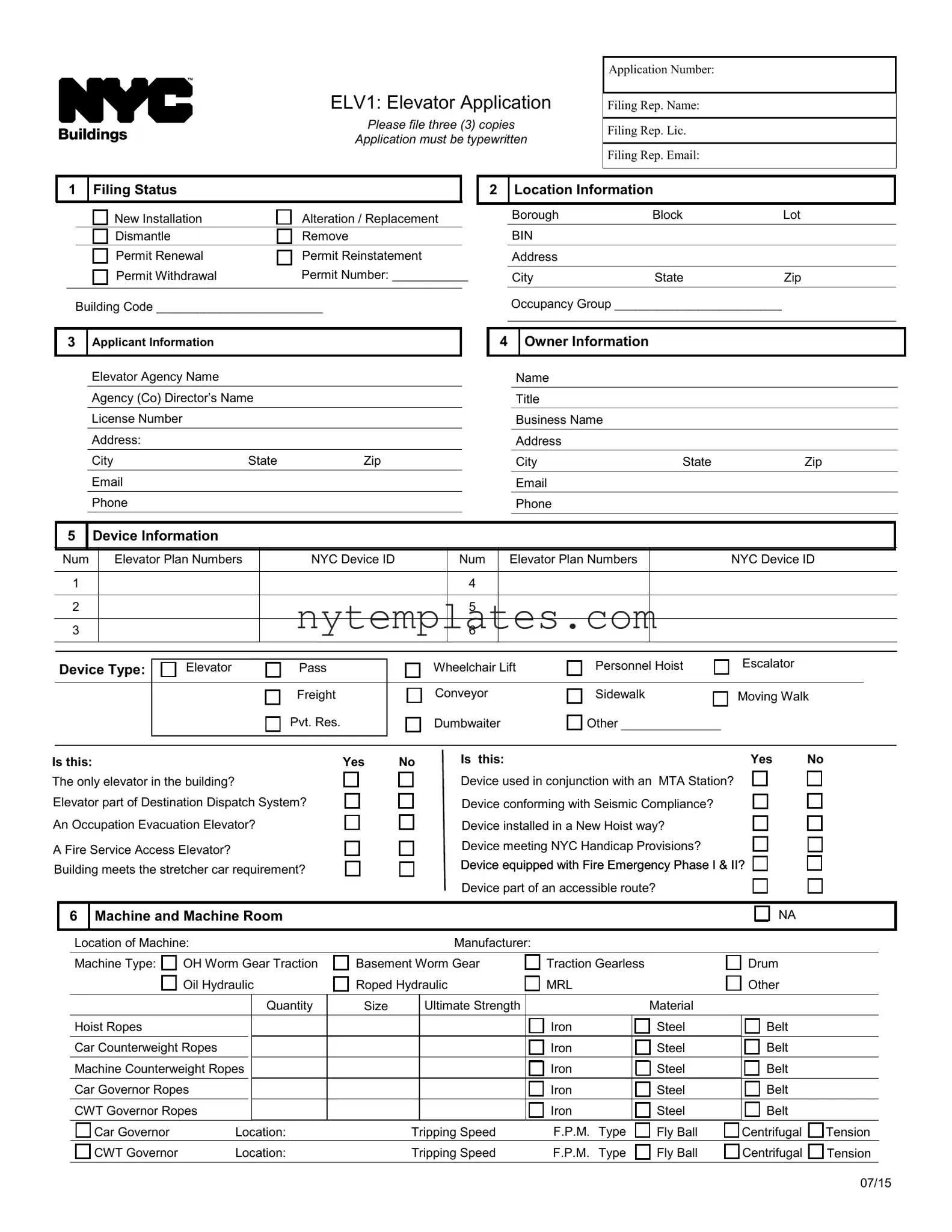
Preview - Nyc Buildings Elv1 Form
ELV1: Elevator Application
Please file three (3) copies
Application must be typewritten
Application Number:
Filing Rep. Name:
Filing Rep. Lic.
Filing Rep. Email:
1 Filing Status
|
New Installation |
Alteration / Replacement |
|
|
Dismantle |
Remove |
|
|
Permit Renewal |
Permit Reinstatement |
|
|
Permit Withdrawal |
Permit Number: ___________ |
|
|
|
|
|
Building Code ________________________
3Applicant Information
Elevator Agency Name Agency (Co) Director’s Name License Number
Address:
City |
State |
Zip |
|
|
|
Phone |
|
|
2 Location Information
Borough |
Block |
Lot |
BIN |
|
|
Address |
|
|
City |
State |
Zip |
Occupancy Group ________________________
4 Owner Information
Name
Title
Business Name
Address
City |
State |
Zip |
|
|
|
Phone |
|
|
5 |
|
Device Information |
|
|
|
|
|
Num |
|
Elevator Plan Numbers |
NYC Device ID |
Num |
Elevator Plan Numbers |
NYC Device ID |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wheelchair Lift |
Personnel Hoist |
Escalator |
|
Device Type: |
|
|
Elevator |
|
Pass |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Freight |
Conveyor |
Sidewalk |
Moving Walk |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Pvt. Res. |
Dumbwaiter |
Other ________________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is this: |
Yes |
The only elevator in the building? |
|
Elevator part of Destination Dispatch System? |
|
An Occupation Evacuation Elevator? |
|
A Fire Service Access Elevator? |
|
Building meets the stretcher car requirement? |
|
No |
Is this: |
Yes |
No |
|
Device used in conjunction with an |
MTA Station? |
|
|
Device conforming with Seismic Compliance? |
|
|
|
Device installed in a New Hoist way? |
|
|
|
Device meeting NYC Handicap Provisions? |
|
|
|
Device equipped with Fire Emergency Phase I & II? |
|
|
|
Device part of an accessible route? |
|
|
6 |
Machine and Machine Room |
|
|
|
|
|
|
|
|
|
|
NA |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Location of Machine: |
|
|
Manufacturer: |
|
|
|
|
|
|
|
|
||||||
|
Machine Type: |
OH Worm Gear Traction |
Basement Worm Gear |
Traction Gearless |
|
Drum |
|
|
||||||||||
|
|
|
Oil Hydraulic |
Roped Hydraulic |
MRL |
|
|
|
|
Other |
|
|
||||||
|
|
|
|
|
Quantity |
Size |
|
Ultimate Strength |
|
|
|
|
|
|
Material |
|
|
|
|
Hoist Ropes |
|
|
|
|
|
|
|
|
Iron |
|
|
|
Steel |
Belt |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Car Counterweight Ropes |
|
|
|
|
|
|
Iron |
|
|
|
Steel |
Belt |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Machine Counterweight Ropes |
|
|
|
|
|
|
Iron |
|
|
|
Steel |
Belt |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Car Governor Ropes |
|
|
|
|
|
|
Iron |
|
|
|
Steel |
Belt |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CWT Governor Ropes |
|
|
|
|
|
|
Iron |
|
|
|
Steel |
Belt |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Car Governor |
Location: |
|
Tripping Speed |
F.P.M. |
Type |
Fly Ball |
Centrifugal |
Tension |
|
|||||||
|
|
CWT Governor |
Location: |
|
Tripping Speed |
F.P.M. |
Type |
Fly Ball |
Centrifugal |
Tension |
|
|||||||
07/15
ELV1 |
PAGE 2 |
7Location Information Please provide the same information as in section 2
Borough |
Block |
LOT |
BIN |
8 |
General Information |
|
|
NA |
|
||
|
|
|
|
|
|
|
|
|
Types of Motive Power |
|
|
|
|
|
|
|
Elevator |
AC |
DC |
Main Supply |
AC |
DC |
|
|
Travel from Floor: |
|
|
to floor: |
|
|
|
|
Total travel |
(ft): |
|
|
Number of Stops: |
|
|
|
Capacity:(lbs) |
|
|
Speed: (FPM) |
|
||
|
Elevator Control |
|
|
|
|
|
|
|
Resistance |
|
|
|
|||
|
Generator Field Control |
Solid State |
|
|
|||
|
Mode of Operation |
Automatic P.B. |
Constant Pressure |
||||
|
Top Emergency Exit Min Area |
sq.in Min Side |
|
in |
|||
|
Glass Car |
|
|
Glass Hoistway |
|
||
|
Atrium Elevator |
|
|
|
|
|
|
9 |
Cars and Counterweight |
|
NA |
|
|
|
|
|
|
|
|
|
|
|
Car Inside Dimensions: |
feet |
in by |
feet |
in |
|
|
Car Inside Area |
|
Sq. feet: |
|
|
|
|
|
|
|
|
|
|
|
Car Safety Type: |
|
|
|
|
|
|
Instantaneous |
|
Flexible Guide |
Gradual WC |
|
|
|
|
|
|
|
|
|
|
Counterweight Safety Type: |
|
|
|
|
|
|
Instantaneous |
|
Flexible Guide |
Gradual WC |
|
|
|
|
|
|
|
|
|
|
Car Opening: |
|
|
|
|
|
|
Door |
|
Gate |
|
|
|
|
|
|
|
|
|
|
|
Operation: |
|
|
|
|
|
|
Manual |
|
Power |
|
|
|
|
|
|
|
|
|
|
|
Contact Type |
|
Manufacturer |
|
|
|
|
|
|
|
|
|
|
|
10 |
|
Hoist way Opening |
|
NA |
11 |
Pit and Buffers |
|
|
|
|
NA |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Door |
|
Gate |
|
|
|
|
|
|
|
|
|
|
Car Buffer: |
Reduced Stroke? |
Yes |
NO |
|
||||||
|
|
|
|
|
|
1 1/2 Hr Fire Rated Construction Type |
|
|
|
|
|
|
|
|
|
Engagement Speed: |
|
|
F.P.M. Stroke |
feet |
|
in |
|
||||||
|
|
|
|
|
|
Operation |
Manual |
|
Power |
|
|
|
|
|
|
Manufacturer: |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Self Closing |
|
Facias |
|
|
|
|
|
|
Type: |
|
|
|
Spring |
Oil |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vision Panel with Grilles |
Vision Panel |
|
|
|
|
|
|
Counterweight Buffer: |
|
|
Reduced Stroke? |
Yes |
|
O |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
||||
|
|
|
|
|
|
|
Interlocks |
|
Locks & Contacts |
|
|
|
|
|
|
Engagement Speed: |
|
|
F.P.M. Stroke |
feet |
|
in |
|
||||||
|
|
|
|
|
|
Interlocks Type: |
|
|
Manufacturer: |
|
|
|
|
|
|
|
|
|
Manufacturer: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of Openings: |
|
|
|
|
|
|
|
|
|
|
|
Type: |
|
|
Spring |
Oil |
|
|
|
|
|
||
|
|
|
|
|
|
Front |
|
|
Side |
|
|
|
|
|
|
|
|
|
Compensation Chain |
|
Length |
|
ft. |
|
|||||
|
|
|
|
|
|
Rear |
|
|
Total: |
|
|
|
|
|
|
|
|
|
Compensation Rope |
|
Length |
|
ft. |
|
|||||
|
|
|
|
|
|
Self Closing Emergency Doors in Blind Hoist way |
|
|
|
|
|
|
Counterweight Screen |
|
Yes |
No |
|
|
|
|
|
||||||||
|
|
|
|
|
|
Interlock in Blind Hoist way |
|
|
|
|
|
|
|
|
|
|
Occupied Space Below |
|
Yes |
No |
|
|
|
|
|
||||
|
12 |
|
Personnel Hoist Information |
NA |
13 |
Escalator Information |
NA |
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Hoist car manufacturer |
|
|
|
|
|
Escalator manufacturer |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Hoist Mast manufacturer |
|
|
|
|
|
|
|
|
Speed |
|
|
|
Rise |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Hoist Safety manufacturer |
|
|
|
|
|
|
|
Width |
|
|
|
Angle |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hoist car dimensions: |
|
|
|
|
|
|
|
Capacity |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hoist car capacity |
|
|
|
|
|
|
|
|
|
Number of flat steps |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hoist Safety Capacity |
|
|
|
|
|
|
|
|
|
|
Brake Torque |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Hoist Safety Expiration Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hoist Counterweighted |
Yes |
No |
|
|
|
|
|
|
Flame/Heat/Smoke protection provided? |
Yes |
No |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Speed |
|
Rise |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
14 |
|
Insurance Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
General Liability |
|
|
|
Company |
|
|
|
|
|
|
|
|
Expiration Date |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
Workers’ Compensation |
|
Certificate/Policy No. |
|
|
Expiration Date |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
Disability |
|
|
|
Certificate/Policy No. |
|
|
Expiration Date |
|
|
|
|
|
|
|||||||||||
07/15
ELV1 |
PAGE 3 |
15Location Information Please provide the same information as in section 2
Borough |
Block |
LOT |
BIN |
16Description of Work: For more space, please AI1 Additional Information
17 |
Statements and Signatures |
|
|
|
|
|
|
|
Falsification of any statement is a misdemeanor and is punishable by a fine or |
Applicant Name |
|
|
imprisonment, or both. It is unlawful to give to a city employee, or for a city employee |
|
|
|
to accept, any benefit, monetary or otherwise, either as a gratuity for properly |
Signature |
Date |
|
performing the job or in exchange for special consideration. Violation is punishable |
|
|
|
|
|
|
|
|
|
|
|
by imprisonment or fine or both. I understand that if I am found after hearing to have |
|
|
|
knowingly or negligently made a false statement or to have knowingly or negligently |
|
|
|
falsified or allowed to be falsified any certificate, form, signed statement, application, |
|
|
|
report or certification of the correction of a violation required under the provisions of |
|
|
|
this code or of a rule of any agency, I may be barred from filing further applications |
|
|
|
or documents with the Department. |
P.E. / R.A. Name (please print) |
|
|
Replacement / Modification Statement |
||
|
|
|
|
|
I am filing this Replacement/Modification Application for consideration under |
|
|
|
Operations Policy and Procedures Notice # 26/90. I certify that no electrical or |
|
|
|
mechanical tests need to be performed in conjunction with this work. |
Signature |
Date |
|
I have assumed responsibility for making inspections during the progress and |
||
|
|
|
|
|
upon completion of the indicated work. Upon completion I will file Form ELV3 to |
|
|
|
sign off on the completed work and to remove all applicable violations. |
|
|
|
P.E. / R.A. Seal |
(apply seal, then sign and date over seal) |
|
|
|
||
18
Fee Information
Estimated Cost: $
Fee Exempt (Proof Required):
New Building Application (Submit Permit)
Internal Use Only
Fee Estimator
Fee Due: |
$ |
|
Fee Estimator Name: |
|
Civil Penalty (If Applicable) : |
$ |
|
Signature: |
Date: |
Total Fee Due: |
$ |
|
|
|
Approvals |
|
|
|
|
Examined and Recommended for Approval: |
|
Approved: |
|
|
Examiner Name: |
|
|
Assistant Commissioner’s Signature: |
|
Signature: |
|
Date: |
|
|
07/15
Form Characteristics
| Fact Name | Fact Details |
|---|---|
| Application Copies | The ELV1 form requires three copies to be filed for processing. |
| Filing Requirements | Applications must be typewritten to ensure clarity and legibility. |
| Device Information | The form collects detailed information about the elevator, including its type and safety features. |
| Governing Laws | This form is governed by the New York City Building Code and related regulations. |
More PDF Templates
Hr Connect Nyc Doe Health Benefits - Through the NYCAP ESS tool, employees can easily view, enroll in, or update their direct deposit and benefits enrollment, ensuring their financial and health coverage details are current.
Ny State Tax Rate - Designated for both retirees visiting client services in person and those sending documents via mail.