Fillable New York Ps 409 Form in PDF
The New York PS 409 form, also known as the Opt-out Attestation Form, is an important document for employees participating in the New York State Health Insurance Program (NYSHIP). This form allows eligible employees to opt out of NYSHIP coverage if they have other employer-sponsored health insurance. By completing the PS 409, employees can receive a financial incentive—$1,000 for waiving individual coverage or $3,000 for waiving family coverage. To qualify, employees must attest that they have alternative health insurance in place as of the opt-out effective date. The form requires basic personal information, including the employee's name, address, and details about their other health insurance coverage. Additionally, it emphasizes the importance of keeping the information up to date, as any changes could affect eligibility. Employees can enroll in the Opt-out Program either when they become newly eligible or during the Annual Option Transfer Period. Understanding the requirements and ensuring timely submission of the PS 409 is crucial for those looking to benefit from this program.
Preview - New York Ps 409 Form
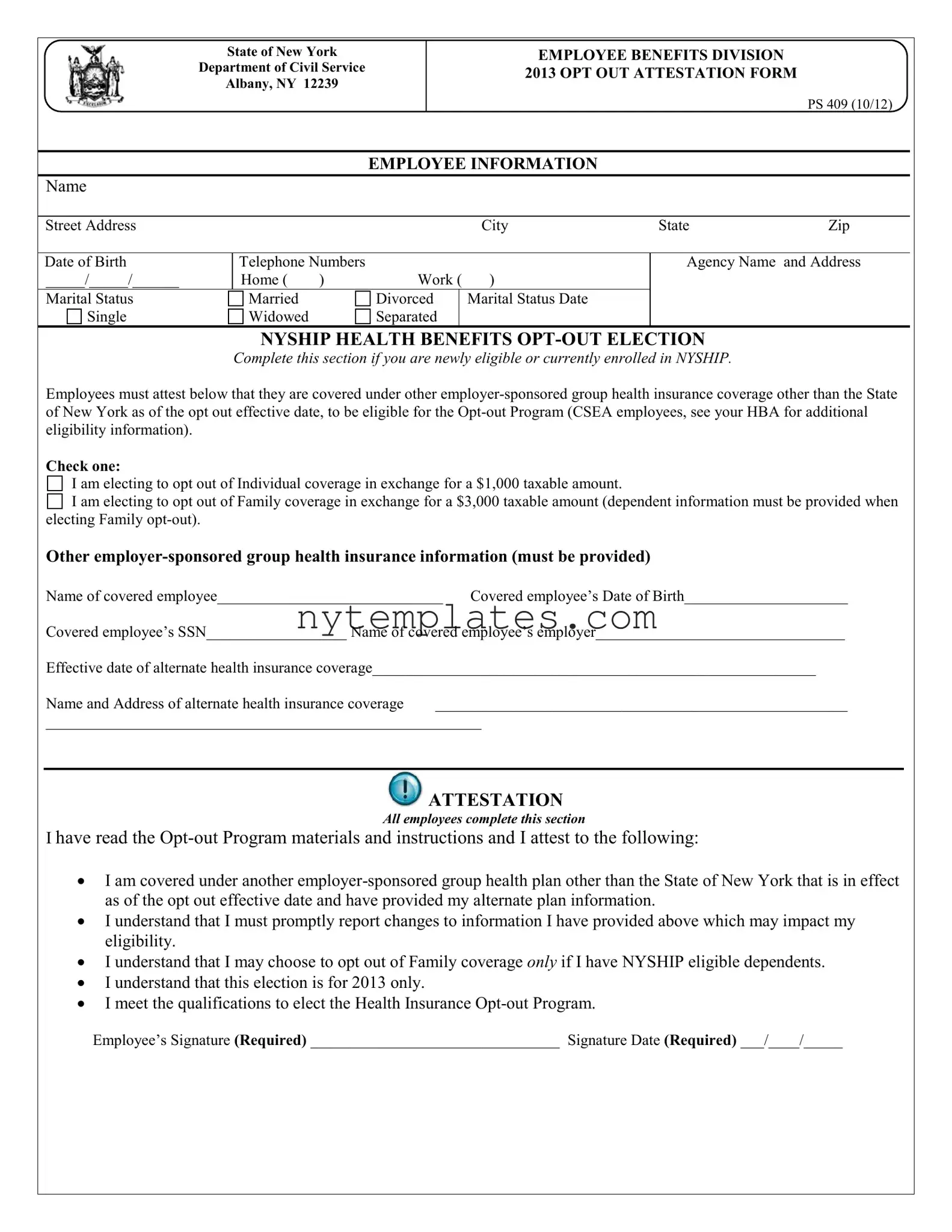
State of New York
Department of Civil Service
Albany, NY 12239
EMPLOYEE BENEFITS DIVISION 2013 OPT OUT ATTESTATION FORM
PS 409 (10/12)
EMPLOYEE INFORMATION
Name
Street Address |
City |
State |
Zip |
Date of Birth |
Telephone Numbers |
|
|
|
|
_____/_____/______ |
Home ( |
) |
Work ( |
) |
|
Marital Status |
Married |
|
Divorced |
|
Marital Status Date |
Single |
Widowed |
|
Separated |
|
|
|
|
|
|
|
|
Agency Name and Address
NYSHIP HEALTH BENEFITS
Complete this section if you are newly eligible or currently enrolled in NYSHIP.
Employees must attest below that they are covered under other
Check one:
I am electing to opt out of Individual coverage in exchange for a $1,000 taxable amount.

 I am electing to opt out of Family coverage in exchange for a $3,000 taxable amount (dependent information must be provided when electing Family
I am electing to opt out of Family coverage in exchange for a $3,000 taxable amount (dependent information must be provided when electing Family
Other
Name of covered employee_____________________________ Covered employee’s Date of Birth_____________________
Covered employee’s SSN__________________ Name of covered employee’s employer________________________________
Effective date of alternate health insurance coverage_________________________________________________________
Name and Address of alternate health insurance coverage _____________________________________________________
________________________________________________________
 ATTESTATION
ATTESTATION
All employees complete this section
I have read the
•I am covered under another
•I understand that I must promptly report changes to information I have provided above which may impact my eligibility.
•I understand that I may choose to opt out of Family coverage only if I have NYSHIP eligible dependents.
•I understand that this election is for 2013 only.
•I meet the qualifications to elect the Health Insurance
Employee’s Signature (Required) ________________________________ Signature Date (Required) ___/____/_____
NYS Department of Civil Service |
Attestation Form |
|
Albany, NY 12239 |
Page 2 |
– PS 409 (10/12) |
Employees who can demonstrate and attest to having other
There are two circumstances when employees may elect to opt out of coverage; as newly eligible for the
INSTRUCTIONS:
Newly eligible employees: Employees may enroll in the
Current enrollees: Eligible enrollees may elect the
During
By signing the
The information you provide on this application is requested in accordance with Section 163 of New York State Civil Service Law for the principal purpose of enabling the Department of Civil Service to process your request concerning health insurance coverage. This information will be used in accordance with Section 96
(1)of the Personal Privacy Protection Law, particularly subdivisions (b), (e) and (f). Failure to provide the information requested may interfere with our ability to comply with your request. This information will be maintained by the Director of the Employee Benefits Division, NYS Department of Civil Service, Albany, NY 12239. For information concerning the Personal Protection Law, call (518)
or
This form is invalid if it is not signed and submitted along with a completed PS 404.
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | The PS 409 form is governed by Section 163 of the New York State Civil Service Law. |
| Purpose | This form allows employees to opt out of the New York State Health Insurance Program (NYSHIP) in exchange for a cash incentive. |
| Incentive Amounts | Employees opting out of Individual coverage receive $1,000, while those opting out of Family coverage receive $3,000. |
| Eligibility Requirements | To be eligible, employees must have other employer-sponsored group health insurance and must have been enrolled in NYSHIP prior to April 1st of the previous plan year. |
| Enrollment Periods | Newly eligible employees can enroll at their first date of NYSHIP eligibility, while current enrollees may do so during the Annual Option Transfer Period. |
| Qualifying Events | Employees who experience a qualifying event may withdraw their opt-out election and enroll in a health insurance plan mid-year. |
| Submission Requirements | The form must be signed and submitted along with a completed PS 404 Enrollment Form to be valid. |
| Tax Implications | The incentive amounts received for opting out are considered taxable income and will be credited to bi-weekly paychecks. |
| Contact Information | For questions regarding the form or health insurance programs, employees can contact the Agency Health Benefits Administrator or the Department of Civil Service. |
More PDF Templates
Property Registration Nyc - Specify if the unit is part of the DHS or HRA shelter system to streamline the registration process.
Nys Tax Exempt Form Hotel - Designed for U.S., New York State, or local government workers, this document facilitates tax-free hotel accommodations.
Ny State Tax Rate - Part of the financial tools available to NYCERS members to manage their retirement benefits effectively.