Fillable New York Nurse 1 Form in PDF
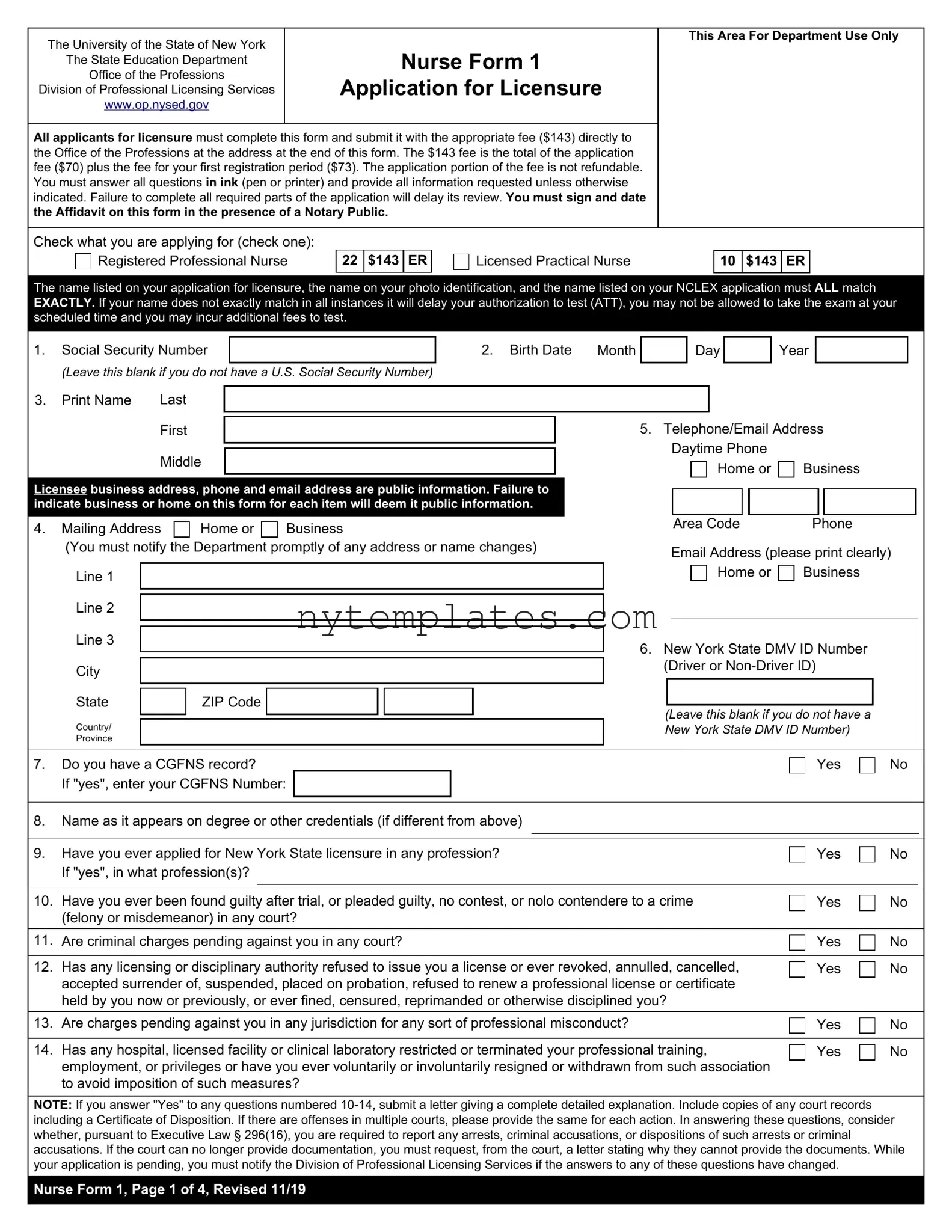
The New York Nurse 1 form is an essential document for anyone seeking licensure as a nurse in New York State. This form must be completed and submitted along with a fee of $143, which covers both the application and initial registration. It requires applicants to provide personal details such as their Social Security number, date of birth, and contact information. Careful attention is needed when filling out the form, as all names must match exactly across various documents, including photo ID and NCLEX applications. Incomplete applications can lead to delays in processing, so it's crucial to answer all questions thoroughly and accurately. Additionally, the form includes sections addressing prior criminal history, professional misconduct, and child support obligations, making it important for applicants to be transparent about their backgrounds. Notably, notarization is required for the affidavit section, ensuring the authenticity of the information provided. Understanding the requirements of the New York Nurse 1 form can streamline the application process and help aspiring nurses move forward in their careers.
Preview - New York Nurse 1 Form
The University of the State of New York |
|
|
|
|
|
|
|
This Area For Department Use Only |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
The State Education Department |
|
|
Nurse Form 1 |
|
|
|
|
|
||||||
|
Office of the Professions |
|
|
|
|
|
|
|
||||||
|
|
Application for Licensure |
|
|
|
|
|
|||||||
Division of Professional Licensing Services |
|
|
|
|
|
|
||||||||
|
|
www.op.nysed.gov |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All applicants for licensure must complete this form and submit it with the appropriate fee ($143) directly to |
|
|
|
|
|
|||||||||
the Office of the Professions at the address at the end of this form. The $143 fee is the total of the application |
|
|
|
|
|
|||||||||
fee ($70) plus the fee for your first registration period ($73). The application portion of the fee is not refundable. |
|
|
|
|
|
|||||||||
You must answer all questions in ink (pen or printer) and provide all information requested unless otherwise |
|
|
|
|
|
|||||||||
indicated. Failure to complete all required parts of the application will delay its review. You must sign and date |
|
|
|
|
|
|||||||||
the Affidavit on this form in the presence of a Notary Public. |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check what you are applying for (check one): |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Registered Professional Nurse |
22 |
$143 |
ER |
|
|
Licensed Practical Nurse |
|
10 |
$143 |
ER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The name listed on your application for licensure, the name on your photo identification, and the name listed on your NCLEX application must ALL match EXACTLY. If your name does not exactly match in all instances it will delay your authorization to test (ATT), you may not be allowed to take the exam at your scheduled time and you may incur additional fees to test.
1. |
Social Security Number |
|
|
|
|
|
|
|
|
2. Birth Date |
Month |
|
|
|
|
|
Day |
|
|
|
|
Year |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
(Leave this blank if you do not have a U.S. Social Security Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
3. |
Print Name |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Telephone/Email Address |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Daytime Phone |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Middle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home or |
|
|
Business |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Licensee business address, phone and email address are public information. Failure to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
indicate business or home on this form for each item will deem it public information. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Mailing Address |
Home or |
|
|
|
Business |
|
|
|
|
|
Area Code |
|
|
|
Phone |
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
(You must notify the Department promptly of any address or name changes) |
|
|
|
|
Email Address (please print clearly) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Line 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home or |
|
|
Business |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Line 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. New York State DMV ID Number |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Driver or |
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Leave this blank if you do not have a |
|
|
|
|
||||||||||||||||||||||
|
Country/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New York State DMV ID Number) |
|
|
|
|
|||||||||||||||||
|
Province |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Do you have a CGFNS record? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
If "yes", enter your CGFNS Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Name as it appears on degree or other credentials (if different from above) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
9. |
Have you ever applied for New York State licensure in any profession? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
||||||||||||||||||||||||
|
If "yes", in what profession(s)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
10. |
Have you ever been found guilty after trial, or pleaded guilty, no contest, or nolo contendere to a crime |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
Yes |
|
No |
|
|||||||||||||||||||||||||||||||||||||
|
(felony or misdemeanor) in any court? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
11. |
Are criminal charges pending against you in any court? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
12. |
Has any licensing or disciplinary authority refused to issue you a license or ever revoked, annulled, cancelled, |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
Yes |
|
No |
|
|||||||||||||||||||||||||||||||||||||
|
accepted surrender of, suspended, placed on probation, refused to renew a professional license or certificate |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
held by you now or previously, or ever fined, censured, reprimanded or otherwise disciplined you? |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
13. |
Are charges pending against you in any jurisdiction for any sort of professional misconduct? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
14. |
Has any hospital, licensed facility or clinical laboratory restricted or terminated your professional training, |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
Yes |
|
No |
|
|||||||||||||||||||||||||||||||||||||
|
employment, or privileges or have you ever voluntarily or involuntarily resigned or withdrawn from such association |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
to avoid imposition of such measures? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
NOTE: If you answer "Yes" to any questions numbered
Nurse Form 1, Page 1 of 4, Revised 11/19
15. Do you now hold, or have you ever held, a license or certificate to practice any profession in any state or jurisdiction? |
|
Yes |
|
|
No |
If yes, list each license/certificate, state or jurisdiction and provide appropriate information in the columns below. A Form 3 or Nursys |
|
||||
license verification (for states reporting to Nursys) must be submitted for each professional license/certificate listed unless it is a license/certificate issued by the New York State Education Department. See the Applicant instructions on Form 3 for specific information about completing and submitting the form.
Professional Title
State or Jurisdiction
Date License/Certificate |
License/Certificate |
Issued |
Number |
|
|
Limitations
on License/Certificate
16.You must complete all information for all schools/colleges/universities attended or your application will be considered incomplete. Note: If you are applying for licensure as a licensed practical nurse and you did not graduate from a New York State approved nursing program, you must submit a copy of your high school or secondary school diploma or transcript in the original language with your Form 1. If you were educated outside the U.S. or a Canadian province other than Quebec with a BN, BSN or BScN after
January 1, 2015), submit a copy of your nursing diploma in the original language.
Elementary or Primary School - Please complete the section below with details about your elementary or primary school. Attach additional sheets if you attended multiple schools. Any missing information will be considered an incomplete application.
Name of School
City |
State/Province |
|
|
|
|
|
|
|
Country |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of years attended |
Attendance from |
|
|
to |
|
|
|
|
Completion date |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mo. |
|
yr. |
|
mo. |
|
yr. |
|
|
|
mo. |
|
yr. |
|
|
High School/Secondary School or Equivalency Diploma Issuer - Please complete the section below with details about your high school/secondary school or equivalency diploma issuer. Attach additional sheets if you attended multiple schools. Any missing information will be considered an incomplete application.
Name of School
City |
State/Province |
|
|
|
|
|
|
|
Country |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of years attended |
Attendance from |
|
|
to |
|
|
|
|
Completion date |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mo. |
|
yr. |
|
mo. |
|
yr. |
|
|
|
mo. |
|
yr. |
|
|
Nurse Program - Please complete the section below with details about your nursing program. Attach additional sheets if you attended multiple programs. Any missing information will be considered an incomplete application.
Name of School
City |
|
State/Province |
|
|
|
|
|
|
Country |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major/Concentration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Number of years attended |
|
Attendance from |
|
|
to |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
mo. |
|
yr. |
|
mo. |
|
yr. |
|
|
|
|
|||
Title of Degree/Diploma/Certificate awarded (in original language) |
|
|
|
|
|
|
|
|
|
Or |
|
Still in progress |
|||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Date Degree/Diploma/Certificate awarded |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
mo. |
|
yr. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Postsecondary Education - Please complete the section below with details about your postsecondary education. Attach additional sheets if you attended multiple schools. Any missing information will be considered an incomplete application.
Name of School
City |
|
State/Province |
|
|
|
|
|
|
Country |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major/Concentration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Number of years attended |
|
Attendance from |
|
|
to |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
mo. |
|
yr. |
|
mo. |
|
yr. |
|
|
|
|
|||
Title of Degree/Diploma/Certificate awarded (in original language) |
|
|
|
|
|
|
|
|
|
Or |
|
Still in progress |
|||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Date Degree/Diploma/Certificate awarded |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
mo. |
|
yr. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Nurse Form 1, Page 2 of 4, Revised 11/19
17.If you have ever taken the SBTP, NCLEX, or a
State or Territory* |
|
Profession |
|
Exam Name |
|
Exam Date |
|
If Granted, License No. |
|
|
|
|
|
|
|
|
|
State or Territory* |
|
Profession |
|
Exam Name |
|
Exam Date |
|
If Granted, License No. |
|
|
|
|
|
|
|
|
|
State or Territory* |
|
Profession |
|
Exam Name |
|
Exam Date |
|
If Granted, License No. |
|
|
|
|
|
|
|
|
|
State or Territory* |
|
Profession |
|
Exam Name |
|
Exam Date |
|
If Granted, License No. |
*If you took the NCLEX or SBTP Examination, send Form 3 to the state in which you passed the licensing examination or request verification from Nursys.
18.Child Support Obligation
Everyone applying for a professional license, permit, or registration, or any renewal thereof, must certify that, as of the date of the filing, she or he is, or is not, under an obligation to pay child support*. Individuals who are four months or more in arrears in child support or who have failed to comply with a summons, subpoena or warrant relating to a paternity or child support proceeding may be subject to suspension of their business, professional, drivers and/or recreational licenses and permits. The intentional submission of false written statements for the purpose of frustrating or defeating the lawful enforcement of support obligations is punishable under section 175.35 of the Penal Law.
You must complete this section before we can issue the credential for which you have applied. Individuals who are not in compliance with their obligation to pay child support can be issued a credential for no more than six months in order to comply with their child support obligations.
CHECK ONLY A OR B BELOW. If you check B, you must check one of the five statements listed below it.
A
 I am not under an obligation to pay child support;
I am not under an obligation to pay child support;
Or
B
 I am under an obligation to pay child support and (please check only one of the following)
I am under an obligation to pay child support and (please check only one of the following)

 I am current and am not four months or more in arrears in the payment of child support; or,
I am current and am not four months or more in arrears in the payment of child support; or,

 I am making payments by income execution or by court agreed payment plan or by a plan agreed to by the parties; or,
I am making payments by income execution or by court agreed payment plan or by a plan agreed to by the parties; or,

 The child support obligation is the subject of a pending court proceeding; or,
The child support obligation is the subject of a pending court proceeding; or,

 I am receiving public assistance or supplemental security income; or,
I am receiving public assistance or supplemental security income; or, 
 None of the above four statements apply.
None of the above four statements apply.
*New York State General Obligations Law, section
19.Citizenship/Immigration Status
Federal law and the Regulations of the Commissioner of Education (8 NYCRR §59.4) limit the issuance of professional licenses, registrations and limited permits to United States citizens or qualified aliens. To comply with Federal law and Commissioner’s regulation, you must complete this section of this form and check the appropriate box below which indicates your citizenship/immigration status.
I am:
A. A United States citizen or National.
B. An alien lawfully admitted for permanent residence in the United States.

 C. An alien granted asylum under Section 208 of the Immigration and Nationality Act.
C. An alien granted asylum under Section 208 of the Immigration and Nationality Act.

 D. A refugee granted asylum under Section 207 of the Immigration and Nationality Act.
D. A refugee granted asylum under Section 207 of the Immigration and Nationality Act.
E. An alien paroled into the United States under Section 212 (d)(5) of the Immigration and Nationality Act for a period of at least 1 year.
F. An alien whose deportation is being withheld under Section 241 (b)(3) of the Immigration and Nationality Act.

 G. An alien granted conditional entry pursuant to Section 203 (a)(7) of the Immigration and Nationality Act as in effect prior to April 1980.
G. An alien granted conditional entry pursuant to Section 203 (a)(7) of the Immigration and Nationality Act as in effect prior to April 1980.

 H. Non Immigrant (Temporarily in U.S.) Please list Visa type or immigration status or attach a copy of your passport if you are not required to have a Visa to enter the United States
H. Non Immigrant (Temporarily in U.S.) Please list Visa type or immigration status or attach a copy of your passport if you are not required to have a Visa to enter the United States
I. I am an alien not unlawfully present in the United States pursuant to the Deferred Action for Childhood Arrivals (DACA) relief or similar relief from deportation. Please specify
J. I do not reside in the United States.
If you checked any of the boxes from
QUESTIONS ABOUT YOUR IMMIGRATION STATUS AND WHETHER OR NOT IT IS A QUALIFYING STATUS UNDER FEDERAL LAW SHOULD BE DIRECTED TO THE U.S. CITIZENSHIP AND IMMIGRATION SERVICES (USCIS) BY CALLING
OR VISIT THE USCIS WEBSITE.
Nurse Form 1, Page 3 of 4, Revised 11/19
20. Child Abuse Identification and Reporting Coursework Requirement - RN Applicants Only (check one)

 I graduated from a NYS registered program and completed the child abuse identification training as part of my studies.
I graduated from a NYS registered program and completed the child abuse identification training as part of my studies.

 I completed the child abuse coursework and have enclosed a certificate of completion from an approved provider
I completed the child abuse coursework and have enclosed a certificate of completion from an approved provider

 I completed the child abuse coursework online and the approved provider will report that to you electronically.
I completed the child abuse coursework online and the approved provider will report that to you electronically. 
 I am filing for an exemption to the requirement and have enclosed the Certification of Exemption (Form 1CE).
I am filing for an exemption to the requirement and have enclosed the Certification of Exemption (Form 1CE).
21. Infection Control Training Requirement (check one)

 I graduated from a NYS registered licensure qualifying program within the last four years and completed the infection control training during my studies.
I graduated from a NYS registered licensure qualifying program within the last four years and completed the infection control training during my studies.

 I completed the infection control training within the last four years and have enclosed a certificate of completion from an approved provider.
I completed the infection control training within the last four years and have enclosed a certificate of completion from an approved provider.

 I completed the infection control training online within the last four years and the approved provider will report that to you electronically.
I completed the infection control training online within the last four years and the approved provider will report that to you electronically.

 I am filing for an exemption to the requirement and have enclosed an Attestation of Infection Control Training (Form 1IC).
I am filing for an exemption to the requirement and have enclosed an Attestation of Infection Control Training (Form 1IC).
22. Reasonable Testing Accommodations for Individuals with Disabilities. (check if applicable)
I have been diagnosed as having a disability and require special testing accommodations and am submitting the Request for Reasonable Testing Accommodations form. I understand that I will not be able to test until I submit the appropriate documentation and am approved to test with accommodations. (Visit the Office of the Professions' website for information on obtaining the form.)
23.Gender and Ethnicity (This item is optional)
Information on gender and ethnicity is sought solely to allow the New York State Education Department to collect and analyze data concerning diversity in the licensed professions. The ethnic and gender data you provide will be used only for statistical, research, and program evaluation purposes. It will not be released to the public. This information has absolutely no bearing on your qualification for
licensure. |
Gender |
|
Male |
|
Female |
|
|
|
|
|
|
|
|
|
Ethnicity |
|
White (not Hispanic) |
|
Black (not Hispanic) |
|
Asian |
|
Hispanic |
|
Native American |
||
|
|
|
|
|
|
||||||||
24. Education Program Review
I give permission to the New York State Education Department to release my examination results to my professional school for the confidential purposes of program review and institution research and planning. I may rescind this authority at any time by notifying the
Division of Professional Licensing Services in writing. |
|
Yes |
|
No |
Please initial |
25.Affidavit with Acknowledgement (Notarization required)
Applicant
I declare and affirm that the statements made in this application, including accompanying documents, are true, complete and correct. I understand that any false or misleading information in, or in connection with, my application may be cause for denial or loss of licensure and may result in criminal prosecution. This form must be signed and dated in the presence of a Notary Public.
Applicant's Signature |
|
|
|
|
|
|
|
Date |
|||
Notary |
|
|
|
|
|
|
|
|
|
||
State of |
|
|
|
|
County of |
|
|
|
|
||
On the |
|
day of |
|
|
in the year |
|
|
before me, the above signed, |
|||
|
|
|
|
|
|
|
|
|
|
|
|
personally appeared |
|
|
|
|
|
|
, personally known to me or proved to me on the basis |
||||
|
|
|
|
|
Applicant name |
|
|
|
|||
of satisfactory evidence to be the individual whose name is subscribed to this application and acknowledged to me that he/she executed
the application and swore that the statements made by him/her in the application and all supporting materials are true, complete, and
correct.
Notary Public's Signature
Notary Stamp
Notary ID number |
Expiration Date |
If you are submitting an initial Form 1, mail this form and appropriate fee to: New York State Education Department, Office of the Professions, PO Box 22063, Albany, NY 12201, U.S.A.. DO NOT SEND CASH. Make check or money order payable to the New York State Education Department.
If the Department has requested an updated Form 1, mail this form to: New York State Education Department, Office of the Professions, Nurse Unit, 89 Washington Avenue, Albany, NY
Nurse Form 1, Page 4 of 4, Revised 11/19
Form Characteristics
| Fact Name | Details |
|---|---|
| Governing Body | The New York State Education Department oversees the Nurse Form 1. |
| Application Fee | The total fee for application is $143, which includes a $70 application fee and a $73 registration fee. |
| Refund Policy | The application fee is non-refundable once submitted. |
| Signature Requirement | Applicants must sign the affidavit in the presence of a Notary Public. |
| Name Consistency | All names on the application, ID, and NCLEX must match exactly to avoid delays. |
| Social Security Number | Applicants must provide their Social Security Number, or leave it blank if they do not have one. |
| Child Support Obligation | Applicants must certify their compliance with child support obligations as per New York State General Obligations Law, section 3-503. |
| Citizenship Requirement | Federal law limits licensure to U.S. citizens or qualified aliens, as outlined in 8 NYCRR §59.4. |
| Education Verification | Applicants must list all educational institutions attended; incomplete information will render the application incomplete. |
| Submission Instructions | The completed form must be mailed to the appropriate address, along with the fee, if applicable. |
More PDF Templates
Utilities in Business - Completing the form requires detailed business information, including contacts and identification numbers, for proper processing.
Rp5217 - This document is a vital component of the legal framework governing real estate transactions within New York City's unique market.