Fillable New York Claim Form in PDF
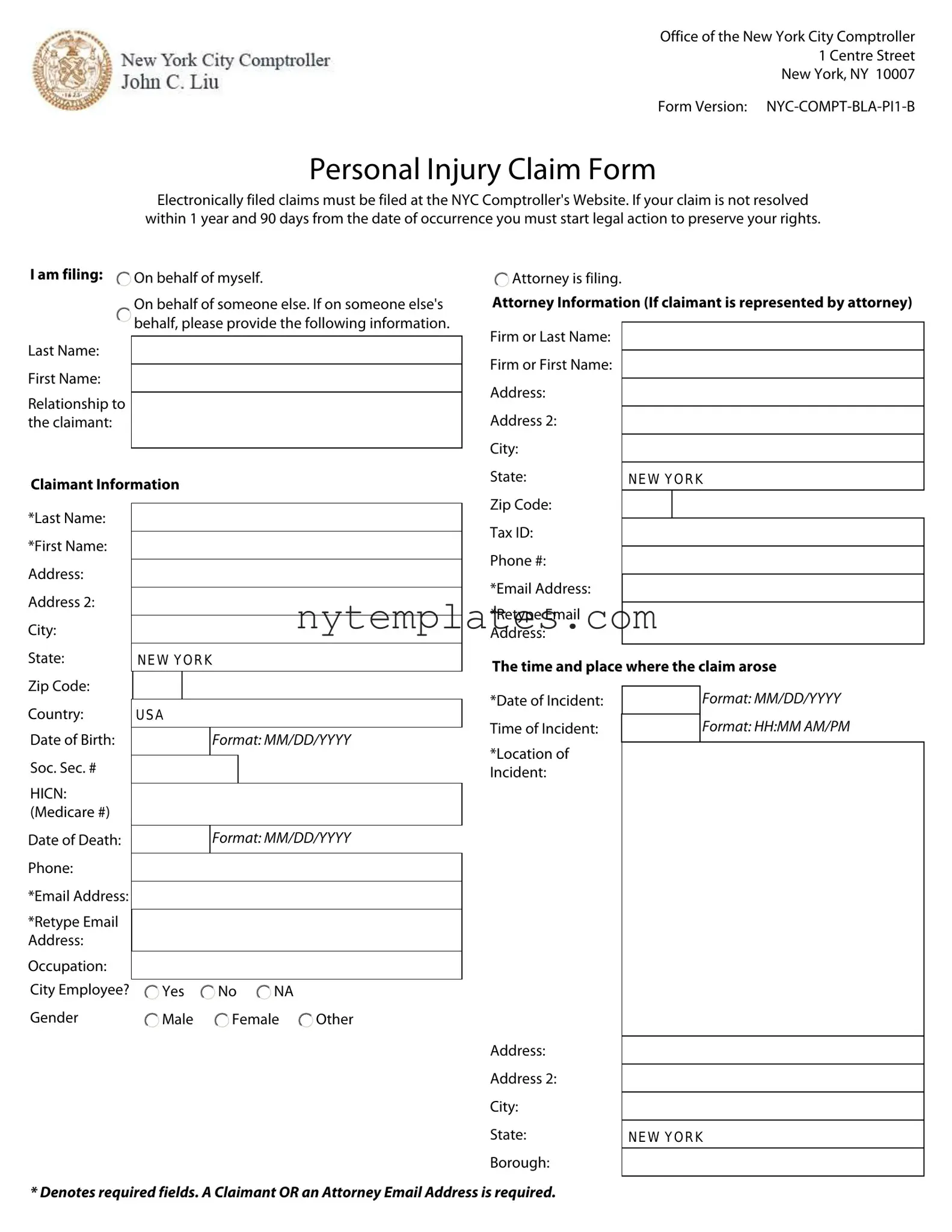
Navigating the New York Claim form can seem daunting, but understanding its key components is essential for anyone looking to file a personal injury claim in the city. This form, officially titled the NYC-COMPT-BLA-PI1-B, is designed to collect vital information about the claimant, the incident, and the damages incurred. Individuals can file on their own behalf or on behalf of someone else, requiring specific details about the claimant, such as their name, relationship to the filer, and contact information. Essential fields include the date and location of the incident, a description of how the claim arose, and the items of damage or injuries claimed, often accompanied by dollar amounts. Medical information, including treatment dates and hospital details, is also critical, as is any employment information if lost wages are being claimed. Witness information may further support the claim, while details about any involved vehicles and insurance information help to clarify the context of the incident. Importantly, the form emphasizes that claims must be filed electronically through the NYC Comptroller's website, and it highlights the necessity of initiating legal action if a claim remains unresolved for over a year and 90 days. By familiarizing oneself with these aspects, claimants can better prepare their submissions and ensure their rights are protected.
Preview - New York Claim Form
Office of the New York City Comptroller
1 Centre Street
New York, NY 10007
Form Version:
Personal Injury Claim Form
Electronically filed claims must be filed at the NYC Comptroller's Website. If your claim is not resolved within 1 year and 90 days from the date of occurrence you must start legal action to preserve your rights.
I am filing:  On behalf of myself.
On behalf of myself.
On behalf of someone else. If on someone else's  behalf, please provide the following information.
behalf, please provide the following information.
 Attorney is filing.
Attorney is filing.
Attorney Information (If claimant is represented by attorney)
Last Name:
First Name:
Relationship to the claimant:
Claimant Information
Firm or Last Name: Firm or First Name: Address:
Address 2:
City:
State:
NEW YORK
*Last Name:
*First Name:
Address:
Address 2:
City:
State:
Zip Code:
Country:
Date of Birth:
Soc. Sec. #
HICN: (Medicare #)
Date of Death: Phone:
*Email Address:
*Retype Email Address:
Occupation:
City Employee?
Gender
NEW YORK
USA
Format: MM/DD/YYYY
Format: MM/DD/YYYY
 Yes
Yes  No
No  NA
NA
 Male
Male  Female
Female  Other
Other
Zip Code: Tax ID: Phone #: *Email Address:
*Retype Email
Address:
The time and place where the claim arose
*Date of Incident: |
|
Format: MM/DD/YYYY |
|
Time of Incident: |
|
|
Format: HH:MM AM/PM |
|
|
||
|
|
|
|
*Location of |
|
|
|
Incident: |
|
|
|
Address: |
|
Address 2: |
|
City: |
|
State: |
NEW YORK |
Borough: |
|
* Denotes required fields. A Claimant OR an Attorney Email Address is required.
Office of the New York City Comptroller
1 Centre Street
New York, NY 10007
*Manner in which claim arose:
* Denotes required field.
Office of the New York City Comptroller
1 Centre Street
New York, NY 10007
The items of damage or injuries claimed are (include dollar amounts):
Medical Information
Office of the New York City Comptroller
1 Centre Street
New York, NY 10007
Witness 1 Information
1st Treatment Date:
Hospital/Name:
Address:
Address 2:
City:
State:
Zip Code:
Date Treated in Emergency Room:
Format: MM/DD/YYYY
NEW YORK
Format: MM/DD/YYYY
Last Name:
First Name:
Address
Address 2:
City:
State: |
NEW YORK |
Zip Code:
Witness 2 Information
Was claimant taken to hospital by |
Yes |
No |
NA |
an ambulance? |
|
|
|
Employment Information (If claiming lost wages)
Last Name:
First Name:
Address
Employer's Name:
Address
Address 2:
City:
State:
Zip Code:
Work Days Lost:
Amount Earned Weekly:
NEW YORK
Address 2:
City:
State: |
NEW YORK |
Zip Code:
Witness 3 Information
Last Name:
First Name:
Address
Treating Physician Information
Last Name:
First Name:
Address:
Address 2:
City:
State: |
NEW YORK |
Zip Code:
Address 2:
City:
State: |
NEW YORK |
Zip Code:
Witness 4 Information
Last Name:
First Name:
Address
Address 2:
City:
State: |
NEW YORK |
Zip Code:
Office of the New York City Comptroller
1 Centre Street
New York, NY 10007
Complete if claim involves a NYC vehicle
Owner of vehicle claimant was traveling in |
Last Name:
First Name:
Address
Address 2:
City:
State:
Zip Code:
NEW YORK
Last Name:
First Name:
Address
Address 2:
City:
State:
Zip Code:
NEW YORK
Insurance Information
Insurance Company Name:
Address
Address 2:
City:
State:
Zip Code:
Policy #:
Phone #:
NEW YORK
Make, Model, Year of Vehicle:
Plate #:
VIN #:
City vehicle information
Plate #:
City Driver Last
Name:
Description of |
Driver |
Passenger |
City Driver First |
claimant: |
Pedestrian |
Bicyclist |
Name: |
|
|
||
|
Motorcyclist |
Other |
|
Total Amount
Claimed:
The Total Amount Claimed can only be entered once the following required fields are entered:
Claimant Last Name
Claimant First Name
Claimant Email or Attorney Email
Date of Incident
Location of Incident
Manner in which claim arose
Format: Do not include "$" or ",".
I certify that all information contained in this notice is true and correct to the best of my knowledge and belief. I understand that the willful
making of any false statement of material fact herein will subject me to criminal penalties and civil liabilities.
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | The New York Claim form is governed by New York City Administrative Code § 7-201. |
| Filing Method | Claims must be electronically filed at the NYC Comptroller's Website. |
| Time Limit | If unresolved within 1 year and 90 days from the date of occurrence, legal action must be initiated. |
| Required Fields | Certain fields, marked with an asterisk (*), are mandatory for submission of the form. |
| Claimant Information | Claimants can file on their own behalf or on behalf of someone else, with specific details required for each. |
More PDF Templates
Department of Buildings Nyc - Completion and submission of this form by the 15th of the following month are mandatory requirements, underscoring the urgency in complying with administrative procedures.
Prevailing Wage Reporting - The requirement for a detailed breakdown of hours and earnings per day promotes accurate wage calculations.
Nyc General Corporation Tax - It underscores the collaborative nature of tax administration, involving corporations, tax preparers, and government agencies in streamlined processes.