Fillable Ga 4 New York Form in PDF
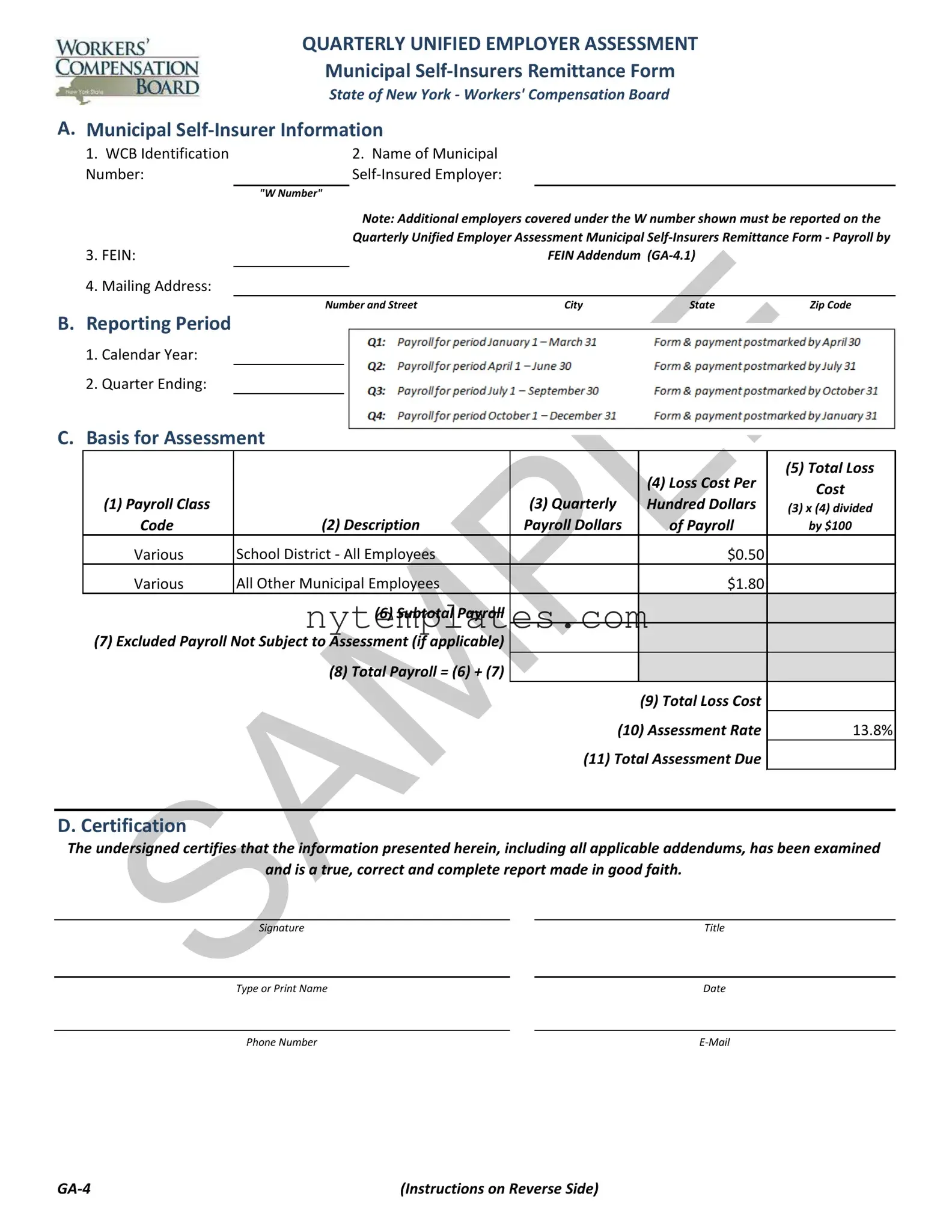
The GA-4 New York form, officially known as the Quarterly Unified Employer Assessment Municipal Self-Insurers Remittance Form, plays a crucial role for municipal self-insured employers in New York. This form must be completed and submitted quarterly, ensuring compliance with state regulations regarding workers' compensation. It gathers essential information such as the WCB Identification Number, the name of the self-insured employer, and the Federal Employer Identification Number (FEIN). Employers must report their total payroll, distinguishing between school districts and other municipal employees, and calculate the corresponding assessment based on established rates. The form also requires a certification statement, affirming the accuracy of the submitted information. Timely submission is vital, as it must be filed within thirty days following the end of each quarter, along with the appropriate payment. Failure to comply can result in penalties, including interest on underpayments and potential revocation of self-insured status. Understanding the intricacies of the GA-4 form is essential for maintaining compliance and avoiding costly repercussions.
Preview - Ga 4 New York Form
QUARTERLY UNIFIED EMPLOYER ASSESSMENT
Municipal
State of New York - Workers' Compensation Board
A. Municipal
1. |
WCB Identification |
|
2. Name of Municipal |
|
|
|
Number: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
"W Number" |
|
|
|
|
|
|
|
Note: Additional employers covered under the W number shown must be reported on the |
|||
|
|
|
Quarterly Unified Employer Assessment Municipal |
|||
3. |
FEIN: |
|
|
FEIN Addendum |
|
|
4. |
Mailing Address: |
|
|
|
|
|
|
|
|
|
|
||
|
|
Number and Street |
City |
State |
Zip Code |
|
B.Reporting Period
1.Calendar Year:
2.Quarter Ending:
C.Basis for Assessment
|
|
|
|
(5) Total Loss |
|
|
|
(4) Loss Cost Per |
Cost |
|
|
(3) Quarterly |
|
|
(1) Payroll Class |
|
Hundred Dollars |
(3) x (4) divided |
|
Code |
(2) Description |
Payroll Dollars |
of Payroll |
by $100 |
Various |
School District - All Employees |
|
$0.50 |
|
Various |
All Other Municipal Employees |
|
$1.80 |
|
|
(6) Subtotal Payroll |
$0 |
|
|
(7) Excluded Payroll Not Subject to Assessment (if applicable) |
|
|
|
|
|
(8) Total Payroll = (6) + (7) |
$0 |
|
|
|
|
|
(9) Total Loss Cost |
|
|
|
(10) Assessment Rate |
13.8% |
|
|
|
(11) Total Assessment Due |
|
|
|
|
|
|
|
D. Certification
The undersigned certifies that the information presented herein, including all applicable addendums, has been examined
and is a true, correct and complete report made in good faith.
Signature |
|
Title |
|
|
|
Type or Print Name |
|
Date |
|
|
|
Phone Number |
|
(Instructions on Reverse Side) |
Instructions for Completing Quarterly Unified Employer Assessment
Municipal
General Instructions
1.The Quarterly Unified Employer Assessment Municipal
2.Additional municipal employers covered under the W number shown must be reported on the Quarterly Unified Employer Assessment Municipal Self- Insurers Remittance Form - Payroll by FEIN Addendum
3.Questions about the form or process should be directed to WCBFinanceOffice@wcb.ny.gov.
4.Checks are to be made payable to the Chair, NYS Workers' Compensation Board.
5.To ensure the proper application of payment please include W Number and applicable quarter on check.
6.This report and corresponding payment, along with applicable addendum, must be submitted quarterly by every municipal employer actively self- insured for workers' compensation. Employers that discontinued their
Submit completed form via
WCBFinanceOffice@wcb.ny.gov
and mail check to address below
Or mail completed form and check to:
New York State Workers’ Compensation Board
328 State Street
Finance Unit, Room 331
Schenectady, NY
Municipal
1.The WCB Identification Number or "W Number" as assigned to the municipal
2.The Name of the Municipal
3.The FEIN, or Federal Employer Identification Number, must be reported for the municipal
4.The full mailing address of the municipal
Basis for Assessment
1.A blended rate for municipal payroll will be used and there is no need to breakout by class.
2.Payroll must be broken out between employers which are school districts and all other municipal employers.
3.Total quarterly payroll associated with either the school district and/or all other types of municipal
4.The loss cost per hundred dollars of payroll for municipal employers and school districts is set annually by the Chair. The rates are shown on the Quarterly Unified Employer Assessment Municipal
5.The total loss cost is determined by multiplying the payroll by the loss cost shown and dividing by $100.
6.Subtotal of payroll reported on the Quarterly Unified Employer Assessment Municipal
7.Excluded payroll not subject to assessment.
8.With limited exception, total payroll should agree with that reported on the Quarterly Combined Withholding, Wage Reporting and Unemployment
|
Insurance Return |
|
please provide reconciliation. No payroll caps are to be applied. |
9. |
Equal to the sum of all of the loss cost by payroll class shown. |
10. |
The assessment rate for the rating period established by the Chair pursuant to WCL Section 151. This can be found on the WCB's website |
|
www.wcb.ny.gov. |
11. |
The total assessment due is equal to the total loss cost multipled by the assessment rate. |
Certification
In accordance with WCL Section 151 the Chair may conduct periodic audits of any
QUARTERLY UNIFIED EMPLOYER ASSESSMENT
Municipal
Payroll by FEIN Addendum
State of New York - Workers' Compensation Board
A. Municipal
|
|
2. Name of |
1. WCB Identification |
|
Municipal Self- |
Number: |
|
Insured Employer: |
|
|
|
|
"W Number" |
|
B.Reporting Period
1.Calendar Year:
2.Quarter Ending:
C.Municipal Employers Covered Under the W Number Shown Above
|
|
|
(4) Excluded |
|
|
(3) Quarterly |
Payroll (if |
(1) FEIN |
(2) Municipal |
Payroll |
applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(5) Subtotal Payroll |
|
|
|
(6) Subtotal Excluded Payroll (if applicable) |
|
|
|
(7) Total Payroll = (5) + (6) |
|
$0 |
|
|
|
|
Instructions for Completing Quarterly Unified Employer Assessment
Municipal
Payroll by FEIN Addendum
General Instructions
1.The Quarterly Unified Employer Assessment Municipal
2.The Quarterly Unified Employer Assessment Municipal
3.The payroll by class code reported on the Quarterly Unified Employer Assessment Municipal
4.Questions about the form or process should be directed to WCBFinanceOffice@wcb.ny.gov.
5.This addendum, if applicable, must be sent quarterly with the Quarterly Unified Employer Assessment Municipal
Municipal
1.The WCB Identification Number or "W number" as assigned to the municipal
2.The Name of the Municipal
Municipal Employers Covered Under the W Number
1.The FEIN, or Federal Employer Identification Number, must be reported for the municipal
2.The municipal
3.Total quarterly payroll associated with the FEIN number.
4.Excluded payroll not subject to assessment.
5.Subtotal of payroll subject to assessment of the Quarterly Unified Employer Assessment Municipal
6.Subtotal of excluded payroll not subject to the assessment of the Quarterly Unified Employer Assessment Municipal
7.Total payroll and excluded payroll if applicable. With limited exception, total payroll should agree with that reported on the Quarterly Combined
Withholding, Wage Reporting and Unemployment Insurance Return
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Purpose | The GA-4 form is used for the Quarterly Unified Employer Assessment Municipal Self-Insurers Remittance in New York. |
| Governing Law | This form is governed by the New York Workers' Compensation Law, specifically Section 151. |
| Filing Frequency | Municipal self-insured employers must complete and submit the GA-4 form quarterly. |
| Submission Deadline | The form must be submitted within thirty days after the end of each quarter. |
| WCB Identification | The form requires the WCB Identification Number, also known as the "W Number," assigned to the municipal self-insurer. |
| FEIN Requirement | The Federal Employer Identification Number (FEIN) must be reported for the municipal self-insurer. |
| Assessment Calculation | The total assessment due is calculated by multiplying the total loss cost by the established assessment rate. |
| Excluded Payroll | Employers can report excluded payroll that is not subject to assessment, if applicable. |
| Certification | The form must be certified by an authorized individual, affirming the accuracy of the information provided. |
More PDF Templates
Nyc 5Ub - Partnerships can deduct a specific exemption from their net business income to calculate the estimated tax.
How to Close a Corporation in Ny - A form to navigate the legal process of altering support conditions or nullifying a child support subpoena.
What Is a Fire Emergency Plan - Outlines the requirements for conducting and documenting evacuation drills, an essential part of the Fire Safety Plan's implementation.